A Tale of Two Shelter Organizations in Approaches to Supporting People that Use Substances
In summary, there are two organizations that I have had recent engagements with that demonstrate the huge gulf in understanding of harm reduction and practice of harm reduction in homelessness support services and housing support services.
Organization One does not allow any person that is suspected of using alcohol or other drugs on property. There is no access to harm reduction supplies or education in Organization One. There remains a perception amongst leadership of Organization One that people need to want to get clean and sober, and that people have to make that choice in their life if they want to get a job and retain housing. “Otherwise, there’s no point in housing ‘em,” remarked the shelter executive.
Organization Two, on the other hand, already distributes harm reduction supplies, provides harm reduction education and is actively involved in harm reduction programming for people that use substances or are involved in sex work. Organization Two is currently looking to integrate a supervised consumption site, begin a Managed Alcohol Program, and support access to safer drug supply, while also exploring alternate models to community-based safer sobering.
True across Organization One and Organization Two is that they both claim to be low barrier, both claim to be ending homelessness, and both believe their approach to engaging with people that use substances is the best approach.
Harm reduction is an evidence-based practice. It even has a journal! Harm reduction literature is clear: harm reduction interventions are demonstrably effective for assisting people that use alcohol or other drugs. The effectiveness has been demonstrated in many settings with different populations, including people experiencing homelessness. In other words, harm reduction is not just an opinion on how to assist people (and entire communities) that are negatively impacted by their use of alcohol or other drugs; it has been proven to work. To reject harm reduction as an idea or practice without reviewing the evidence means the objection to harm reduction is ideological, not based on fact.
Harm reduction embraces core principles. While the articulation of the principles varies between harm reduction organizations and coalitions, and the populations they serve specifically (e.g., people that use substances; people involved with sex work) they generally can be summed up as follows when it comes to substance use:
Pragmatism: we work to reduce the immediate and tangible harms of substance use, rather than embracing an abstract notion of a drug free society.
Focus on harms: we focus on the reduction of harmful consequences of use, which can include a broad array of strategies from access to supplies to change in substance, mode of practice, frequency and/or location.
Autonomy: the decision to use alcohol or drugs is a personal one, and the decision to use comes with the responsibilities associated with it.
Flexibility: actions and possibilities are considered at the individual level, without expectation of a particular course of action in a certain order.
Prioritization of Goals: goals are set at the individual level, with more immediate actions that can reduce the most immediate harms prioritized ahead of longer-term, more future oriented goals.
In developing a harm reduction approach that will work best in any particular shelter environment, it is critical to ensure the voices of people with living experience of substance use are included. Intentionally, marginalized voices such as those that identify as BIPOC, 2SLGBTQ*, gender non-binary, gender non-conforming and differently abled must be included. Harm reduction does not succeed if it is not culturally safe.
In practicing harm reduction within a shelter, workers should be expected to:
· respect the individual and see and support the whole person in achieving optimum wellness as defined by the individual;
· be supportive and conscious of the autonomy of the person engaged in substance use;
· empower shelter guests in making decisions related to their substance use;
· exhibit compassion and express empathy; and,
· collaborate with the shelter guest to develop approaches to reduce harm that are aligned to the needs of the person using substances.
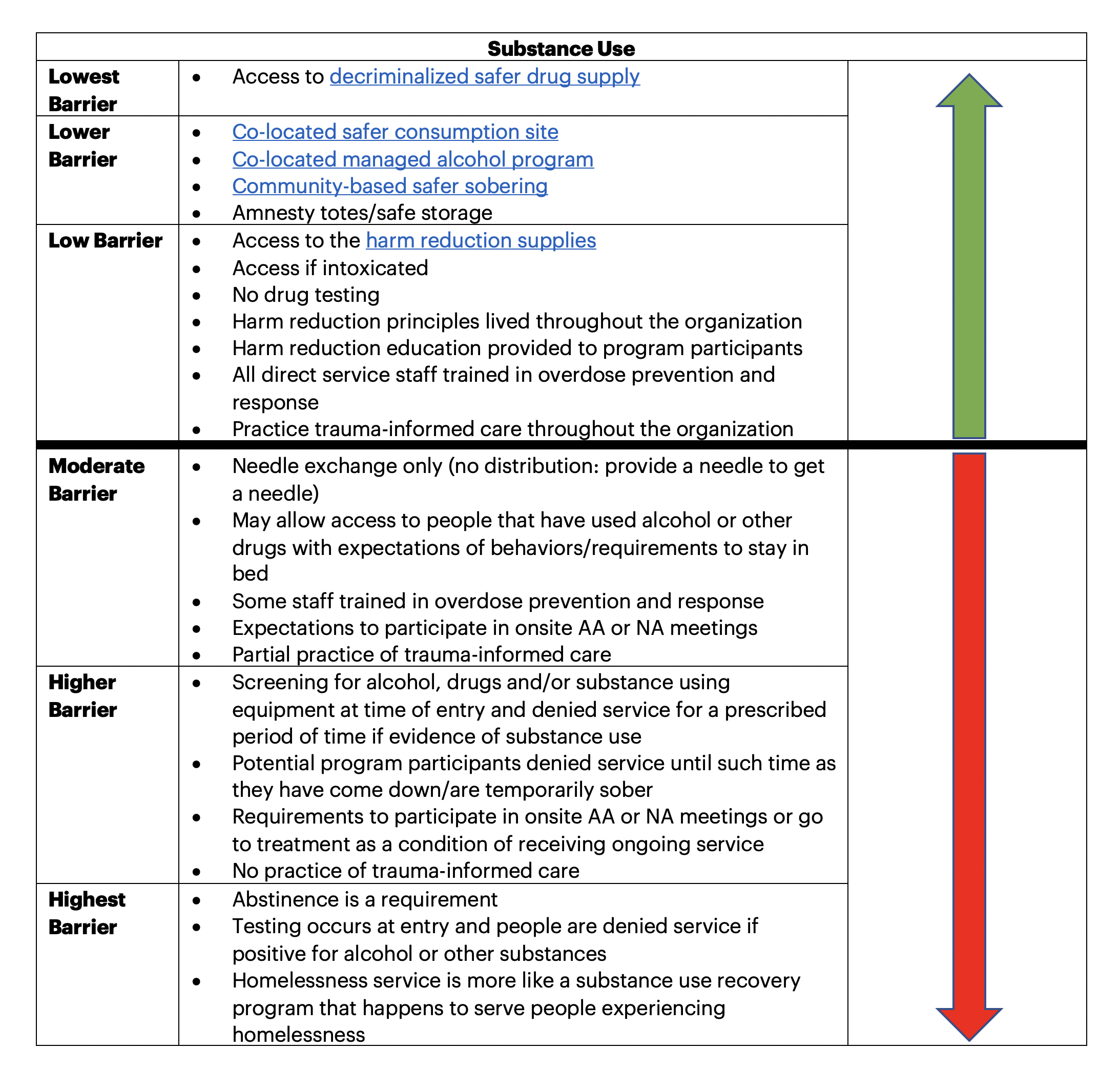
Harm reduction practices exist along a continuum in the delivery of shelter services. I put together this table to demonstrate some of those ideas. (As an aside, consider this table a work in progress that can be updated with more examples of harm reduction practices with people that use substances in a shelter environment.)
Harm reduction is predicated upon meeting people where they are at. For organizations that they are non-judgmental, the provision of harm reduction is relatively straightforward, but for organizations that claim to be non-judgmental but have practices related to drug testing or requiring sobriety, they likely are judgmental. Seeing the whole person and their potential to reduce harm in their lives requires a truly person-centered and hopeful approach to service delivery. Delivering harm reduction is also aligned to a trauma-informed approach to the work, especially if we lean into the connection in many people’s lives between past traumas and current substance use. We must create environments for service that are emotionally, psychologically and physically safe for people that use substances. We should be transparent in our quest for trust-building. We should empower trained peers in the journey to reducing harm and improving wellness. We should give people voice and choice in the services they want and goals they want to pursue. We should appreciate cultural, historical and gender use in substance use and harm reduction.
Harm reduction services to people experiencing homelessness should be coupled with a focus on housing. Results of research by Milaney et al. conclude: Results highlight the importance of concurrently addressing housing instability alongside the provision of harm reduction services. Secure housing with supports can further reduce harm of substance use.
If you are a shelter that is already practicing harm reduction, or a shelter interested in the practice of harm reduction, you may want to check out this resource prepared by Public Health in the City of Toronto. It is a guidance document on the practice of harm reduction in shelters. You may find it helpful to compare shelter practices in your community currently with the 10 Points of Harm Reduction for Shelter Programs. Then look at opportunities for improvement and change that will further lower barriers relative to the population you are serving and your local context.
There are some shelter providers that want to provide a space for people working on sobriety. If there is more than one shelter in the community or a floor/area within the shelter where that can be provided, it may be appropriate to have a small part of the system that requires sobriety. However, let’s explicitly name it as such, provide a policy rationale for doing so, and stop claiming that doing so is lower barrier. Moderate to higher barrier sober sheltering can be integrated into a broader system of care, so long as the most vulnerable people experiencing homelessness have at least one place they can go and be accepted in the community if they use substances. Furthermore, a person seeking a sober shelter should do so because that is what they desire, not because it is the only shelter space available. Our aim should always be to provide a social service, not to exercise social control.
Now back to Organization One and Organization Two. With changes in sheltering practices and demands on shelter services resulting from COVID, I would argue we need to be as low barrier as is operationally possible. Now is not the time for further restrictions on access that will place even more people experiencing homelessness in peril. With homelessness likely to get worse before it gets better, I cringe at the thought of a divide in shelter access that, in essence, is determining a deserving and undeserving population based upon their substance use. Might this mean changes in policy and practice? Yes. Might this mean more training is needed? Yes. Might this mean working with funders and neighbours to help them understand what you are aiming to do? Yes. Might more people stay alive making it possible to house them, support them, and reduce harms associated with their substance use? Yes to that too.